Frequently Asked Questions about PRISM
How does PRISM Compare to RE-AIM? Are they different Frameworks?
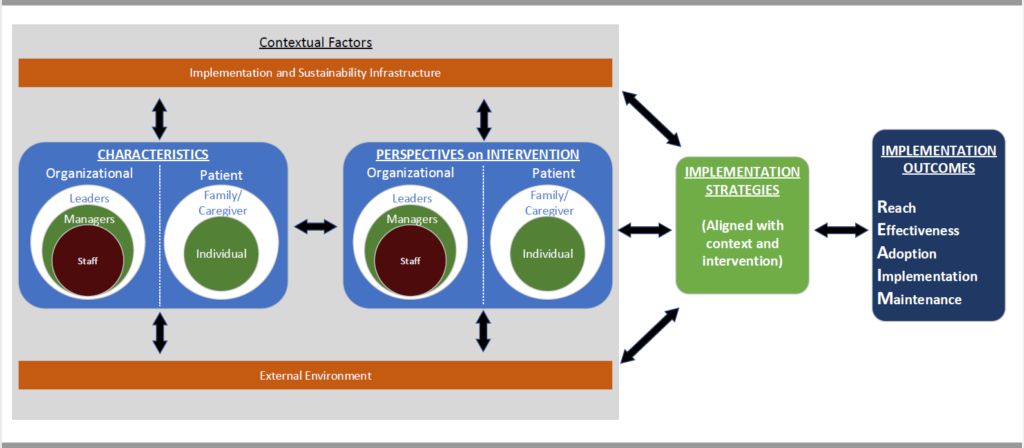
PRISM actually includes RE-AIM. As seen in the Figure below, PRISM adds contextual factors that interact with an intervention (program, practice, policy) and implementation strategies to produce RE-AIM outcomes. IMPORTANTLY: RE-AIM and PRISM are not different frameworks. When possible we encourage use of the full PRISM model because of the additional information and opportunities involved in learning about and addressing context. We recognize that this is not always possible, and in such cases recommend briefly stating why it was not possible or appropriate to use the PRISM context factors.
What are the Key contextual issues or concepts in PRISM?
There are four contextual PRISM domains, each of which is multi-level. These are: (1) Perspectives on the intervention (e.g., history with similar programs, relationships, mental models); (2) Characteristics of implementers, their settings, and those receiving the intervention (patients) (e.g., at citizen, delivery staff, organizational decision makers and community levels); (3) external environment (e.g., policies, distribution of resources, health and social system structure and coverage); and (4) implementation and sustainability infrastructure (e.g., resources, and capacity; staff roles and responsibilities; monitoring and evaluation systems).
Key points about and examples of each of the PRISM domains are below.
Perspectives:
Organizational and staff perspectives on the program (intervention): characteristics such as organizational readiness for the program, the program’s perceived evidence strength, and compatibility with existing workflow.
Patient (recipients) perspectives on the program (intervention): characteristics such as perceptions of the program’s patient-centeredness, patient barriers and service and access, and estimated impact and ease of use.
Characteristics of Implementing Settings; Staff; and Patient and Family recipients
• Organizational characteristics: characteristics that affect organizations’ ability to successfully change behaviors in a given clinical area; for example, clinical leadership, management support and communication; these factors can be considered at the levels of top management, middle managers and delivery staff.
• Patient characteristics: characteristics of the intended patients; for example, age, gender, culture, level of social needs, and health literacy.
External environment: characteristics such as relevant policies, market forces, regulatory environment and community resources.
Implementation and sustainability infrastructure: characteristics such as adopter training and support, dedicated team for implementation, processes such as ongoing audit and feedback, and resources and plans for sustainability.
How Does PRISM Differ From Other Frameworks that
Assess Context ?
There are a large number of similarities across leading D&I frameworks to assess context- e.g., CFIR, EPIS, PARIS, Normalization Process Theory, and PRISM. All focus on both the ‘inner’ (or organizational) and outer (external environment) setting, and all include characteristics of patients or those receiving the intervention, and almost all are multi-level.
PRISM is more focused than most other context frameworks in that it does not attempt to be comprehensive, but rather pragmatic and focuses on domains most likely to impact RE-AIM outcomes. Perhaps the most unique contextual factor in PRISM is the implementation and sustainability infrastructure. This component is critical to institutionalizing the assessment of equitable implementation and outcomes. PRISM is also explicitly intended to be used across program phases- not just during the initial planning stages (other frameworks can of course be used over time as well, but it is an explicit emphasis of PRISM).
Does PRISM Help to Understand, Assess, and Address Health Equity?
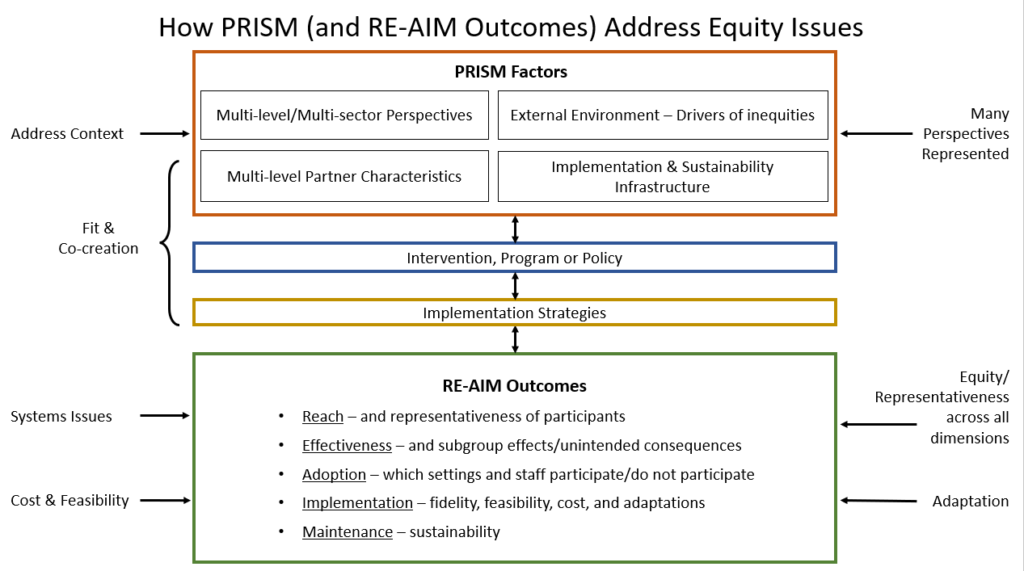
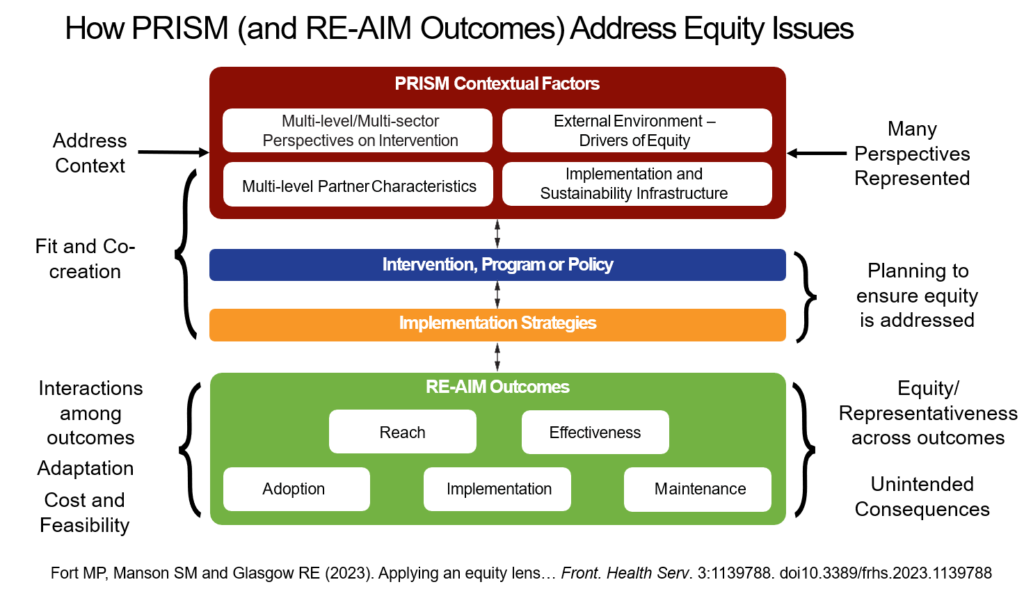
PRISM is a context-oriented implementation science framework that can guide researchers and practitioners to understand, assess, and address structural drivers of health inequities and be positioned to address them during design, implementation, evaluation, and sustainment. The Figure below illustrates key features of PRISM as well as examples of actions to enhance health equity. The center column depicts the key PRISM domains and how they interact with the intervention and implementation strategies to deliver the intervention. The combination and alignment of context, the intervention and the implementation strategies produce the RE-AIM outcomes in the lower part of the figure.
The example actions summarized on the left- and right- side of the figure illustrate how PRISM can be used to enhance equity. Some key opportunities include:
(a) attention to representation of all relevant participants in planning, implementation and evaluation stages of a program;
(b) engagement of participants to co-create and/or adapt the intervention and implementation strategies to fit local context and enhance equity;
(c) assessment of structural drivers of inequity, and capacity and infrastructure needs and resources;
(d) assessment of representativeness (subgroup equity) of results on all RE-AIM outcomes; and
(e) iterative assessment of RE-AIM outcomes to identify equity-enhancing approaches
When should PRISM be used and are there tools
to facilitate its use?
To date, PRISM has been used most often during the planning stages of a program or project (Rabin et al, 2022). However, we strongly encourage use of PRISM domains during the pre-implementation, implementation, and post-implementation (e.g., evaluation and sustainment) phases. Such iterative use can help to help implementation teams guide adaptations and create action plans as well as to evaluate and address any unintended consequences (e.g., exacerbation of inequities) that might occur.
A publicly available web based tool iPRISM to make assessment of and feedback on PRISM issues efficient and confidential is described in Trinkley et al. (2023) and available at prismtool.org
Where Can I Find Examples of the Use of PRISM?
The best use case examples are in the chapter by Trinkley et al. on Applying PRISM in the new book edited by Per Nilsen entitled Implementation science: theory and application (Routledge, 2024).
Articles providing example applications (most are discussed in the above chapter) include:
Guerin et al- in chapter above on implementing a school based occupational health intervention
Pittman et al., 2021: application on use of PRISM in the context of an electronic suicide screening tool:
Pittman, J.O.E., Lindamer, L., Afari, N., Depp, C., Villodas, M., Hamilton, A., et al. (2021a) Implementing eScreening for suicide prevention in VA post-9/11 transition programs using a stepped-wedge, mixed-method, hybrid type-II implementation trial: a study protocol. Implementation Science Communications 2, 46. https://doi.org/10.1186/s43058–021-00142-9.
Trinkley et al., 2021: application or implementing a clinical decision support tool in a large healthcare setting:
Trinkley, K.E., Kroehl, M.E., Kahn, M.G., Allen, L.A., Bennett, T.D., Hale, G., et al. (2021) Applying clinical decision support design best practices with the Practical Robust Implementation and Sustainability Model versus reliance on commercially available clinical decision support tools: randomized controlled trial. JMIR Medical Informatics 9, e24359. https://doi.org/10.2196/24359.
Are There Figures and Tables that Illustrate PRISM?
There are several different figures illustrating PRISM that have been used for different purposes. Below are two of the ones we think are most generally useful.
Check out other figures representing PRISM
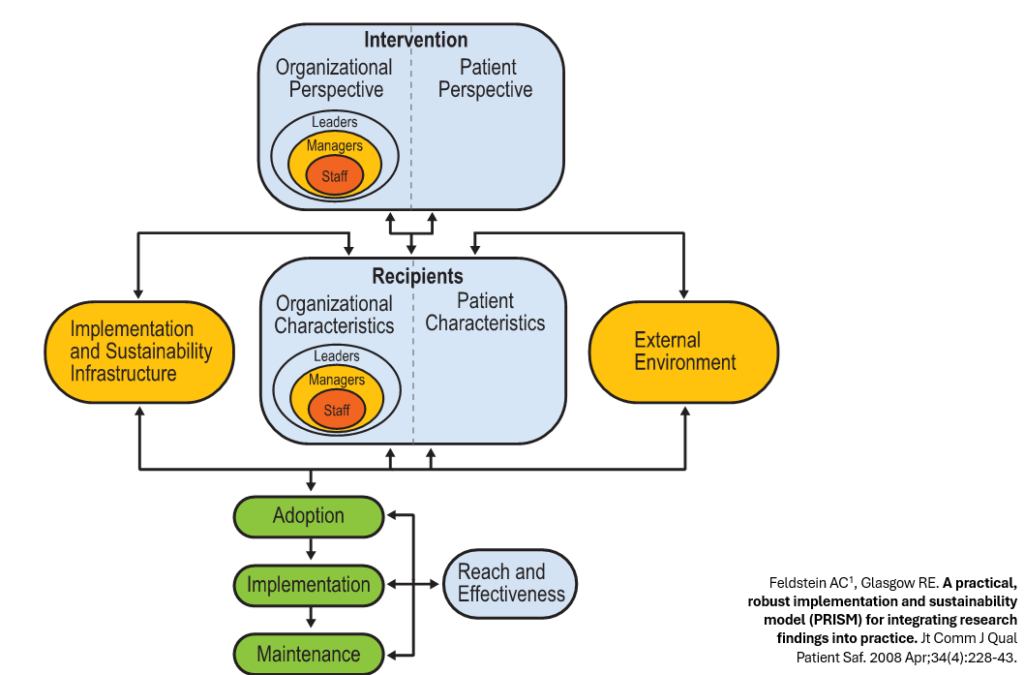
The figure below is the original PRISM figure that was in the first article on PRISM by Feldstein and Glasgow (2008).
The figure below is one of the newest ones and is intended to show how the different PRISM contextual factors, the intervention, and implementation strategies combine to produce implementation (RE-AIM) outcomes using an implementation logic model like display.